Hyperparathyroidism
Hyperparathyroidism is a disorder of the parathyroid glands in which too much parathyroid hormone (PTH) is secreted. Primary hyperparathyroidism means this disorder originates in the parathyroids. One or more enlarged or overactive parathyroid glands secretes too much parathyroid hormone (PTH). Secondary hyperparathyroidism is a condition in which a problem such as kidney failure causes the parathyroids to be overactive. The endocrine surgeons at University Surgeons Associated treat patients with hyperparathyroidism frequently.
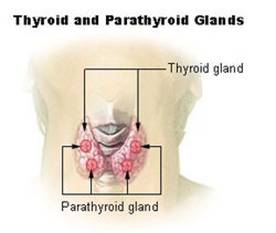
The parathyroid glands are four pea-sized glands located behind the thyroid gland in the neck. Occasionally, a person is born with one or more of the parathyroid glands embedded in the thyroid, in the thymus, or located elsewhere in this area. Though their names are similar, the thyroid and parathyroid glands are entirely different glands, each producing distinct hormones with specific functions. The parathyroid glands secrete parathyroid hormone (PTH), a protein hormone that helps maintain the correct balance of calcium and phosphorus in the body. PTH regulates the release of calcium from bone, absorption of calcium in the intestine, and excretion of calcium in the urine. This controls the level of calcium in the blood. When the level of calcium in the blood falls too low, the parathyroid glands secrete more PTH to restore the blood calcium level.
When parathyroid glands secrete too much hormone, as happens in hyperparathyroidism, the blood calcium level rises. This condition of excessive calcium in the blood, called hypercalcemia, is what usually signals the doctor that something may be wrong with the parathyroid glands. In 85 percent of people with primary hyperparathyroidism, a benign tumor called an adenoma has formed on one of the parathyroid glands, causing it to become overactive. Benign tumors are noncancerous. In most other cases, the excess hormone comes from two or more enlarged parathyroid glands, a condition called hyperplasia. Very rarely, hyperparathyroidism is caused by cancer of a parathyroid gland.
This excess PTH triggers the release of too much calcium into the bloodstream. PTH also lowers blood phosphorus levels by increasing excretion of phosphorus in the urine. Calcium is essential for good health. It plays an important role in bone and tooth development and in maintaining bone strength. Calcium is also important in nerve transmission and muscle contraction. Phosphorus is found in all bodily tissue. It is a main part of every cell with many roles in each. Combined with calcium, phosphorus gives strength and rigidity to your bones and teeth.
In the United States, about 100,000 people develop the disorder each year. Women outnumber men two to one, and risk increases with age. In women 60 years and older, two out of 1,000 will develop hyperparathyroidism each year.The vast majority of cases occur in people with no family history of the disorder. Only about 5 percent of cases can be linked to an inherited problem. Familial multiple endocrine neoplasia type 1 is a rare, inherited syndrome that affects the parathyroids as well as the pancreas and the pituitary gland. Another rare genetic disorder, familial hypocalciuric hypercalcemia, is sometimes confused with typical hyperparathyroidism. Each accounts for about 2 percent of primary hyperparathyroidism cases.
A person with hyperparathyroidism may have severe symptoms, subtle ones, or none at all. Increasingly, routine blood tests that screen for a wide range of conditions, including high calcium levels, are alerting doctors to people who have mild forms of the disorder even though they are symptom-free.
When symptoms do appear, they are often mild and nonspecific, such as a feeling of weakness and fatigue, depression, or aches and pains. With more severe disease, a person may have a loss of appetite, nausea, vomiting, constipation, confusion or impaired thinking and memory, and increased thirst and urination. Patients may have thinning of the bones without symptoms, but with risk of pathologic fractures. Increased calcium and phosphorus excretion in the urine may cause kidney stones or nephrocalcinosis, a condition that can result in kidney failure. Hypercalcemia can also increase the risk for gallstones and gallbladder disease.
Hyperparathyroidism is diagnosed when tests show that blood levels of calcium and parathyroid hormone are too high. Other diseases can cause high blood calcium levels, but only in hyperparathyroidism is the elevated calcium the result of too much parathyroid hormone. A blood test that accurately measures the amount of parathyroid hormone has simplified the diagnosis of hyperparathyroidism.
Once the diagnosis is established, other tests may be done to assess complications. Because high PTH levels can cause bones to weaken from calcium loss, a measurement of bone density can help assess bone loss and the risk of fractures. Abdominal images may reveal the presence of kidney stones and a 24-hour urine collection may provide information on kidney damage, the risk of stone formation, and the risk of familial hypocalciuric hypercalcemia.
Surgery to remove the enlarged gland (or glands) is the main treatment for the disorder and cures it in 95 percent of operations.
Calcimimetics are a new class of drug that turns off secretion of PTH. They have been approved by the Food and Drug Administration for the treatment of hyperparathyroidism secondary to kidney failure with dialysis, and primary hyperparathyroidism caused by parathyroid cancer. They have not been approved for primary hyperparathyroidism, but some physicians have begun prescribing calcimimetics for some patients with this condition. Patients can discuss this class of drug in more detail with their physicians.
Some patients who have mild disease may not need immediate treatment. Patients who are symptom-free, whose blood calcium is only slightly elevated, and whose kidneys and bones are normal may wish to talk with their physicians about long-term monitoring. Periodic monitoring would consist of clinical evaluation, measurement of serum calcium levels, and bone mass measurement. If the patient and physician choose long-term follow-up, the patient should try to drink lots of water, get plenty of exercise, and avoid certain diuretics, such as the thiazides. Immobilization (inability to move) and gastrointestinal illness with vomiting or diarrhea can cause calcium levels to rise. Patients with hyperparathyroidism should seek medical attention if they find themselves immobilized, vomiting, or having diarrhea.
If you have had recurrent kidney stones or been found to have worsening osteoporosis ask your doctor about your calcium level. If you have been found to have an elevated calcium level then check with your doctor about a parathyroid hormone level.
If you've been treated for hyperparathyroidism in the past or if there is a family history of endocrine disorders, it is important that your doctor be aware of that history in evaluating your condition.